
Michael Bevington, the Chair of Trustees at Electrosensitivity UK, outlines the various symptoms and diagnostic methodologies related to Electromagnetic Hypersensitivity (EHS), a condition first diagnosed in 1871
The short-term conscious symptoms of electromagnetic field (EMF) sensitivity or Electromagnetic Hypersensitivity (EHS) have been diagnosed since 1871. These include headaches, heart palpitations, skin rashes, insomnia, anxiety and forgetfulness. EHS is often self-diagnosed but can be verified externally and through tests. Long-term subconscious symptoms, such as cancers, infertility and cardiovascular damage, are shown through comparative general and individual surveys and shielding tests (Table 1).
EHS self-diagnosis
Diagnosing EMF sensitivity is essentially straightforward. From 1733, researchers felt pain and cardiovascular effects from electricity, but not elsewhere. Today, the cause may be WiFi, ‘smart’ meters, mobile phones, wireless watches, or Bluetooth earbuds, where symptoms occur mainly near the device. Some 42% of people self-diagnose hay fever and sunburn, while 25% of 69 subjects accurately self-diagnosed their EMF sensitivity level, as confirmed by altered heart rate variability (HRV).
EHS external diagnosis
Self-diagnosis of EMF sensitivity can be confirmed by others, such as experienced general practitioners taking a clinical history, as from 1871 for telegraph and electricity workers.
Some 96% of Austrian general practitioners accepted adverse EMF symptoms, with 15% suggesting sufferers move house.
EHS diagnosis by general surveys
A general survey in 1932 identified specific EMF symptoms. Another in 1953 found cancers, cataracts, internal bleeding and headaches caused by radar. Surveys near masts from 1996 found increased cancers within 2km, or ten times more cancers in women, and increased irreparable genetic damage.
Surveys also showed long- and short-term symptoms near masts, including greater cognitive impairments in children at a school closer to a mast than in one further away. Children who were more exposed had more ADHD and anxiety problems, and, for maximum exposures, reduced IQ. Surveys since 1979 have also consistently found increased cancer rates near powerlines.
EHS diagnosis by individual assessments
Above a threshold, electrically sensitive people show reactions dependent on frequency but not always field strength. Individual assessments linked EMFs >0.05 V/m, recorded by personal dosimeters, with symptoms and autonomic reactions.
EHS diagnosis by elimination, shielding or negation tests
Diagnostic tests include elimination and comparison of higher and lower EMF exposures through distance or shielding. EMF shielding reduces EHS symptoms. Although silvered nets, developed for military use against electronic warfare, are expensive, they have become an EHS necessity and lifestyle choice for others. Without the EMF cause, there are no symptoms. In 1970, underground shielding from natural EMFs desynchronised people’s circadian rhythms. Shielded visual display units reduced EMF skin rashes. In the Nordic Council of Ministers’ ICD-10 of 2000, EHS or El-Allergy was diagnosed through eliminating symptoms by eliminating EMFs.
Negation testing disrupts magnetoreception. In 1980, blindfolded students showed homeward orientation by sensing geomagnetic fields, but not when disrupted by magnets.
EHS diagnosis by provocation tests
Provocation tests can show EHS with 100% accuracy. Of 25 subjects, 40% showed EMF sensitivity through altered HRV at 0.3% of ICNIRP heating guidelines, confirming that 40% self-rated as moderately or extremely sensitive. Rouleaux blood formations can confirm ten minutes’ provocation using a cordless phone or a wired computer.
Provocation comparisons using masts showed 2.7 increased odds for headaches and 3.7 for migraines at 1-3km, with average exposures of 0.46-0.57 V/m outdoors and 0.04-0.11 V/m indoors, but no symptoms at <0.01 V/m. Case reports near 5G masts in 2023-2024 showed symptoms ceased when subjects moved to areas with less EMF exposure.
Prior screening enables an accurate individual EHS diagnosis. Thus, of 100 participants reporting sensitivity, only 25% identified EMFs accurately. Of these 25, 16 had autonomic neurological changes and were 100% accurate when rechallenged at their most sensitive frequencies, whereas 100% of controls failed.
Inconclusive tests mostly failed to screen participants. Their average results hid accurate individuals. Some excluded 100% of the scores from participants forced to withdraw after EMF harm. In one study, 11% of 63 subjects were accurate, yet the results excluded an unscreened subject with almost perfect detection, arbitrarily allocated to the controls.
EHS diagnosis by threshold and transition tests
EMF perception thresholds among 606 subjects followed two normal distribution bell-shaped curves. The first covered 98% of people; the second, at a much lower level, 2%, all with much higher sensitivity. Among 596 subjects, self-diagnosed EHS significantly matched perception thresholds for 50Hz currents.
For on-off transitions, a subject first screened for relevant frequencies showed 100% accuracy in subconscious biomarkers. Ethically, of course, EMFs, classified by the International Agency for Research on Cancer (IARC) as 2B possible cancer agents, are inappropriate for human tests.
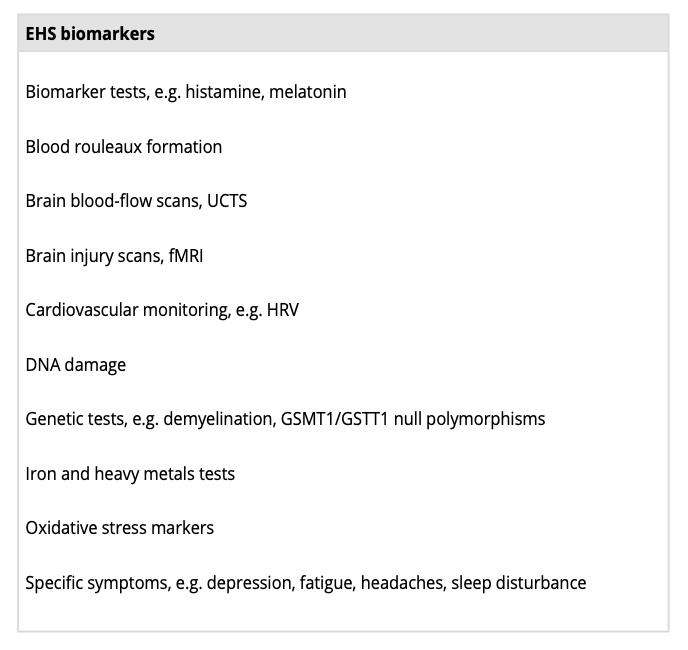
EHS biomarkers
Many biomarkers support EHS diagnoses (Table 2). Using a ‘test battery’ reflects how EMFs affect numerous biological pathways. Nine biomarkers easily diagnosed people with screen dermatitis, but none consistently applied.
Imaging helps. Ultrasonic cerebral tomosphygmography (UCTS) illustrates reduced brain blood (hypoperfusion) in many EHS people, and fMRI shows brain damage. EMFs cause HRV changes, DNA damage, oxidative stress and iron dysregulation and are associated with demyelination and GSMT1/GSTT1 null polymorphisms. These variants are nearly ten times more common in EHS people than others.
Misdiagnosis
Physical EHS is sometimes misdiagnosed as psychological Electrophobia, IEI-EMF, or a nocebo response under the WHO’s arbitrary confusion of these two different conditions. The WHO’s prior psychological conditioning cannot apply to unaware adults, children and animals, all of whom can show EMF sensitivity.





