
Lalit Singh Pukhrambam, PhD, and Ahmed S Ibrahim, PhD from Wayne State University School of Medicine in the U.S. focus here on the importance of combating diabetic retinopathy
Diabetic retinopathy (DR) is a sight-threatening complication of diabetes and the main cause of blindness in the United States among working adults. Initially, DR progresses as a non-proliferative DR (NPDR) which leads to blinding proliferative DR (PDR). Nearly all people with Type 1 Diabetes (T1D) undergo gradual vision loss over a 20-year period of diabetes, and about 20–30% of them progress to the advanced blinding stage of the disease, PDR.
Tight glycaemic management lowers the risk of complications, yet, many diabetic patients develop DR, despite having good glycaemic control. Furthermore, there is no cure or a preventive measure to block PDR. Only recently, over the past decade, with the advent of medicines that block the actions of the vascular endothelial growth factor (VEGF), has considerable progress been made in therapeutic options for PDR.
Nevertheless, not all patients achieve a satisfactory response and many of responders experience frequent invasive intravitreal injections and off-target effects, including increased risk of neuronal toxicity and geographic atrophy. While additional molecular targets, including the plasma kallikrein pathway, lipoprotein-associated phospholipase A2 (Lp-PLA2) and Tie-2, have been identified, with some being clinically evaluated, a critical gap still remains ineffective treatments.
Evidence suggests that targeting DR in the earlier stages, such as mild to moderate NPDR, before permanent damage occurs, would provide long-term benefit. In recent years, our research has focused on the molecular mechanisms of early DR including retinal oxidative stress, mitochondrial dysfunction, mitophagy, inflammation, and premature cell death in diabetes using both in vitro retinal cell cultures and in vivo diabetic rodent models.
Intriguingly, we have discovered a protein called thioredoxin-interacting protein (TXNIP) is strongly induced by diabetes in early DR where it is responsible for mediating cellular oxidative stress, mitophagy, inflammation and premature cell death. Knockdown of TXNIP by intravitreal injection of TXNIP shRNA prevents early molecular defects seen in DR. TXNIP binds to and inhibits the anti-oxidant and thiol-reducing capacity of thioredoxins (Trx) causing cellular redox imbalance and oxidative stress. Trx1 is present in the cytosol and nucleus while Trx2 is located in the mitochondrion. TXNIP is observed in all cellular compartments. Therefore, targeting TXNIP itself or downstream pathways could prevent or slow down the progression of early DR (NPDR) and hence PDR.
Currently, no clinically used, “professional” TXNIP inhibitors exist; however, several FDA-approved medicines have been reported to interfere with TXNIP pathway, but none of them has been used to treat DR. These drugs include amlexanox, tranilast, and romidepsin and they have been extensively studied for their efficacy, toxicity and safety. This consequently leads to saving time and money and may accelerate their entry to experimental clinical trials centred on targeting an over-activated TXNIP system to arrest DR away from their initial use.
Amlexanox is an inhibitor of TANK-Binding Kinase 1 (TBK1), which phosphorylates mitophagy adaptor optineurin and regulates mitophagic flux to lysosomes. In addition, TBK1 also phosphorylates interferon responsive factor 3 (IRF3) and mediates Type 1 interferon expression and inflammation. Tranilast has been shown to inhibit TXNIP and Nod-like NLRP3 inflammasome; therefore, it may help in preventing cellular oxidative stress and innate immune responses.
Therefore, a combination therapy using amlexanox and tranilast may prove to be effective in preventing or slowing down the progression of DR. Recently, we also demonstrated that a combination therapy of SS-31 (a mitochondria-targeted anti-oxidant), amlexanox and tranilast prevents auranofin-induced redox stress, mitochondrial-lysosomal axis dysregulation and proinflammatory pyroptotic cell death in retinal pigment epithelial cells, suggesting that combination therapies may be more effective than a single drug therapy.
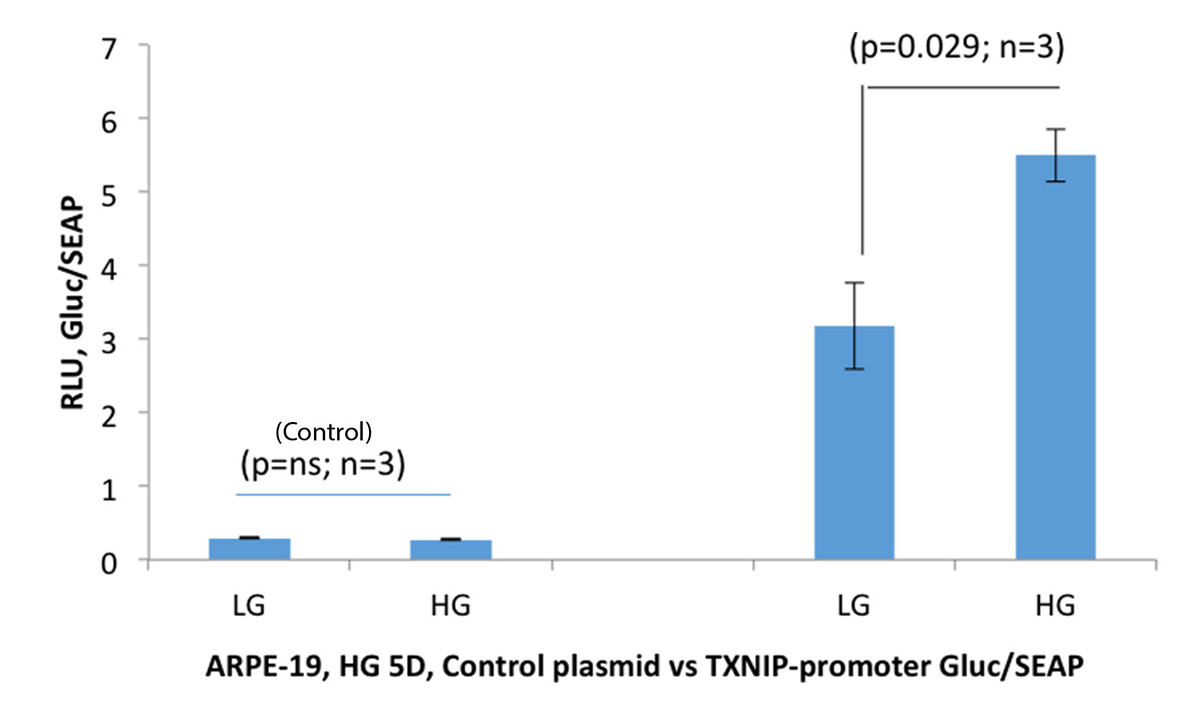
In addition to drug treatment, gene therapy using a TXNIP promoter linked with a neuroprotective factor or an anti-oxidant gene may also be a potential approach for DR treatment. This is because the TXNIP promoter is strongly induced by hyperglycaemia in retinal cells in culture and in diabetic rodent retinas, but not under physiological glucose levels. In addition, the TXNIP promoter is also activated significantly by histone deacetylase inhibitors (HDACi), including suberoylanilide hydroxamic acid (SAHA) or romidepsin.
Therefore, HDACi and TXNIP-promoter gene therapy may also be incorporated in DR therapy for retinal neuroprotective gene expression, which could include pigment epithelium-derived factor (PEDF), glia-derived neurotrophic factor (GDNF), thioredoxin encoded Rod-Derived Cone Viability Factor (RdCVF) and others. These factors are known to be downregulated in DR.
It is currently accepted that neurodegeneration (particularly photoreceptor dysfunction) occurs early in DR before microvascular pathology develops. Therefore, early neuroprotective efforts may constitute a meaningful therapeutical approach to prevent or slow down the progression of late microvascular complications and PDR. Diabetes is a chronic and complex metabolic disease in which PDR develops only after prolonged hyperglycaemic exposure.
Therefore, a window of diabetic duration may exist early to prevent retinal neurovascular dysfunction and progression of PDR; within this time frame, we may devise preventive interventions activating endogenous genes or factors with neuroprotective drugs (preferably orally active drugs) and gene therapy including those mentioned above.
Such a hypothesis is supported by a recent observation, which showed that the expression of retinol binding protein 3 (RBP3), a protein secreted by photoreceptors in the retina, may play a protective role against PDR. RBP3 interacts with glucose transporter Glut1 and reduces excess cellular glucose uptake under hyperglycaemia in diabetics, thus, preventing glucotoxicity in retinal cells including Muller glia and capillary endothelial cells. Those individuals expressing RBP3 do not develop PDR although they have had 50 years of T1D.
In conclusion, new preventive therapies for PDR may be successfully developed by activating endogenous cellular survival mechanisms using drug and gene therapies once a clinical sign of NPDR is observed but before PDR. Such treatments may prevent blindness in diabetic patients.
References
1 Perrone L, Devi TS, Hosoya KI, Terasaki T, Singh LP. Inhibition of TXNIP expression in vivo blocks early pathologies of diabetic retinopathy. Cell Death Dis. 2010 Aug 19;1:e65. PMID: 21364670.
2 Devi TS, Somayajulu M, Kowluru RA, Singh LP. TXNIP regulates mitophagy in retinal Müller cells under high-glucose conditions: implications for diabetic retinopathy. Cell Death Dis. 2017 May 11;8(5):e2777. PMID: 28492550.
3 Lalit PS, Thangal Y, Fayi Y, Takhellambam SD. Potentials of Gene Therapy for Diabetic Retinopathy: The Use of Nucleic Acid Constructs Containing a TXNIP Promoter. Open Access J Ophthalmol. 2018;3(2). PMID: 31106306.
4 Devi TS, Yumnamcha T, Yao F, Somayajulu M, Kowluru RA, Singh LP. TXNIP mediates high glucose-induced mitophagic flux and lysosome enlargement in human retinal pigment epithelial cells. Biol Open. 2019 Apr 25;8(4). PMID: 31023645.
5 Yumnamcha T, Devi TS, Singh LP. Auranofin Mediates Mitochondrial Dysregulation and Inflammatory Cell Death in Human Retinal Pigment Epithelial Cells: Implications of Retinal Neurodegenerative Diseases. Front Neurosci. 2019 Oct 10;13:1065. PMID: 31649499.
6 Yokomizo H, Maeda Y, Park K, Clermont AC, Hernandez SL, et. al., Retinol binding protein 3 is increased in the retina of patients with diabetes resistant to diabetic retinopathy. Sci Transl Med. 2019 Jul 3;11(499). PMID: 31270273.
7 Ibrahim AS, Saleh H, El-Shafey M, Hussein KA, et. al., Targeting of 12/15-Lipoxygenase in retinal endothelial cells, but not in monocytes/macrophages, attenuates high glucose-induced retinal leukostasis. BBA: Mol Cell Biol Lipids. 2017 Jun;1862(6):636-645. PMID: 28351645.
8 Ibrahim AS, Elshafey S, Sellak H, Hussein KA, El-Sherbiny M, et. al., A lipidomic screen of hyperglycemia-treated HRECs links 12/15-Lipoxygenase to microvascular dysfunction during diabetic retinopathy via NADPH oxidase. J Lipid Res. 2015 Mar;56(3):599-611. PMID: 25598081.
Funding
NIH/NEI R01 EY023992 (LSP, OVAS).
NIH/NEI core grant P30EY004068 (LDH, OVAS).
Research to Prevent Blindness (MSJ, OVAS).
American Heart Association Grant 18CDA34080403 to ASI.
Please note: This is a commercial profile








