
In this interview, Mutlu Özcan, Prof. Dr Dr h.c., PhD from the University of Zürich, considers the possibilities concerning reconstructive dentistry and in this vein, digital technologies
Why is the conventional facet of reconstructive dentistry changing?
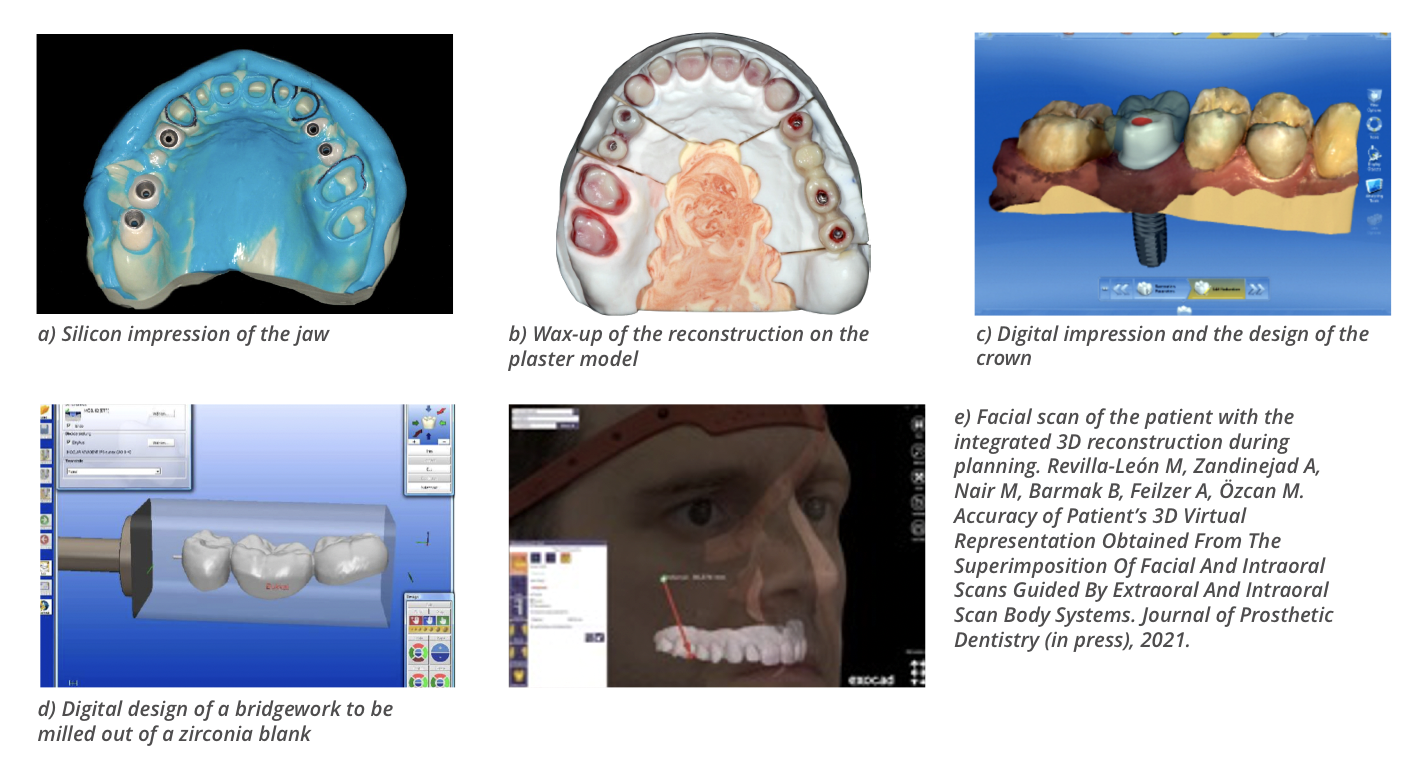
Over the last three decades, advances in the field of dental biomaterials and digital technologies used for the fabrication of tooth, implant- or mucosa-borne dental appliances changed the conventional facet of reconstructive dentistry dramatically. Often reconstructive rehabilitations are accompanied by aesthetic consequences. Therefore, the patient’s expectations should be also met, which requires thorough communication. The conventional sequence for reconstructive treatment planning starts with the collection of diagnostic data comprised of medical and dental history, extraoral and intraoral analysis, diagnostic casts, photographic and video documentation, radiographic evaluation, and diagnostic wax-up performed by the dental technician. In the conventional workflow, impressions are made using hydrocolloid or silicone-based materials, that are then cast in plaster and a facially driven diagnostic wax-up is made. This is then tried in the patient’s mouth, which allows the patient to have realistic expectations of the outcome. Thereafter, interim dental restorations are made for the aesthetic, functional, and phonetic evaluations in the patient’s mouth for a period of time before the definitive restorations are manufactured. Finally, the definitive reconstructions are fabricated through conventional casting procedures and cemented in the mouth. This workflow requires multiple chairside visits to the dentist. Digital technologies, today, allow for creating a digital or in other words, the virtual patient and almost all manual steps in the workflow are substituted by the digital procedures which also significantly decreases the labour delivered by the dental technicians.
What is a digital or virtual patient?
The digital workflows today enable clinicians to combine all possible elements in diagnosis and the data collected during the diagnostic phase to obtain the “digital/virtual patient”. Digital data collection procedures starting with cone-beam computed tomography systems (CBCT), facial and intraoral 3D scans using intraoral scanners (IOS, intraoral photogrammetry digital scans), digital jaw recordings, photographic documentation, and the dynamic recording of the smile and speech can all be integrated using digital tools. Current intraoral scanners devices are based on different, non-contact optical technologies such as confocal microscopy, active and passive stereovision and triangulation, optical coherence tomography, interferometry and phase shift principles to help us obtain virtual diagnostic casts.
The incorporation of digital technologies such as facial scanners facilitates the 3-dimensional (3D) extraoral soft-tissue reconstruction of the patient using anatomic landmarks on the face as reference points. Several 3D facial scanning methodologies have been introduced based on photogrammetry or stereophotogrammetry, laser-beam, and structured light scanning technologies. These face scanners employ active 3D sensors for facial scanning procedures where light patterns are projected onto the extraoral soft tissue of the patient’s face that is captured by a high-resolution camera or cameras using active triangulation. Once the extraoral and intraoral virtual patient representation is achieved, the reconstruction type is digitally planned on the computer screen using specific software programmes; and occlusal adjustments are made and even the shade selection can be accomplished digitally. Before final reconstruction is fabricated, a complete digital workflow involves a direct digital procedure to transfer the patient’s data into a virtual space where digital diagnostic casts are mounted onto a virtual articulator. This procedure requires a virtual facebow transfer that positions the maxillary diagnostic cast in the virtual articulator in its skull-related position, generating a standard coordinate system between patient data and the virtual space. Through this transfer, excursive movements of the jaws that are recorded intraorally are integrated with the virtual patient.
What is the next step to fabricate the reconstructions digitally?
After the jaw relation, smile line, phonetics are established, the reconstruction is designed virtually on the computer screen using digital tools. Software programmes utilising also some tooth libraries allow us to choose the closest tooth morphology and assist us in designing the final reconstruction. Today, we have a large plethora of materials to choose from when it comes to restoring dentition. Almost all of these can be fabricated using computer-aided design and computer-aided manufacturing (CAD-CAM) methods. Such CAD-CAM reconstructions could be either milled from a blank of zirconium dioxide, lithium disilicate, feldspathic ceramics or from resin-based composite materials chairside using robotic devices. Small size reconstructions often can be fabricated in less than an hour and cemented in the patient’s mouth, which decreases multiple visits to the dentist.
What are the current challenges in digital technologies?
One of the most important aspects of reconstructive rehabilitation is to generate an ideal treatment plan and long-lasting reconstructions created, based on detailed data collection. Digital workflows and each step in the process, needs extensive research before full integration in the clinical workflow. The field is very dynamic and is led often by manufacturers. The digital workflow requires costly investments, therefore, fundamental knowledge on the working mechanism of the systems should be considered before purchasing such systems. In that context, one big challenge is the extremely quick pace of implementation of newly introduced digital tools since the lifetime of such digital devices and innovation are getting much shorter. The other challenge is the integration of different dental digital technologies into the same dental CAD software programme as some manufacturers still prefer to use closed systems. Nevertheless, increased accuracy and precision in digital workflows are expected to decrease chairside time and also reduce the labour on both the dental technician and dentist.
Please note: This is a commercial profile








