
Following the first two articles that discussed the treatment of cancer and pain, this third piece will focus on the use of cannabinoids to treat psoriasis and rheumatoid arthritis
Endocannabinoids, as well as several phytocannabinoids, have been shown to influence immune functions, regulating inflammation, autoimmunity, antitumourigenesis, antipathogenic responses and other processes.1 Numerous in vitro and in vivo studies have examined the therapeutic potential of cannabinoid signalling in inflammation-associated diseases (e.g. psoriasis) and attempted to dissect the complex immunological effects of cannabinoids.
Cannabinoids and psoriasis
Psoriasis is a chronic inflammatory disease of the skin, characterised by excessive proliferation of keratinocytes that results in the formation of thickened scaly plaques, itching and inflammatory changes of the epidermis and dermis.2 The underlying pathophysiology involves activation of classes of T-cells and their interaction with dendritic cells and other cells of the innate immune system, including neutrophils and keratinocytes.3
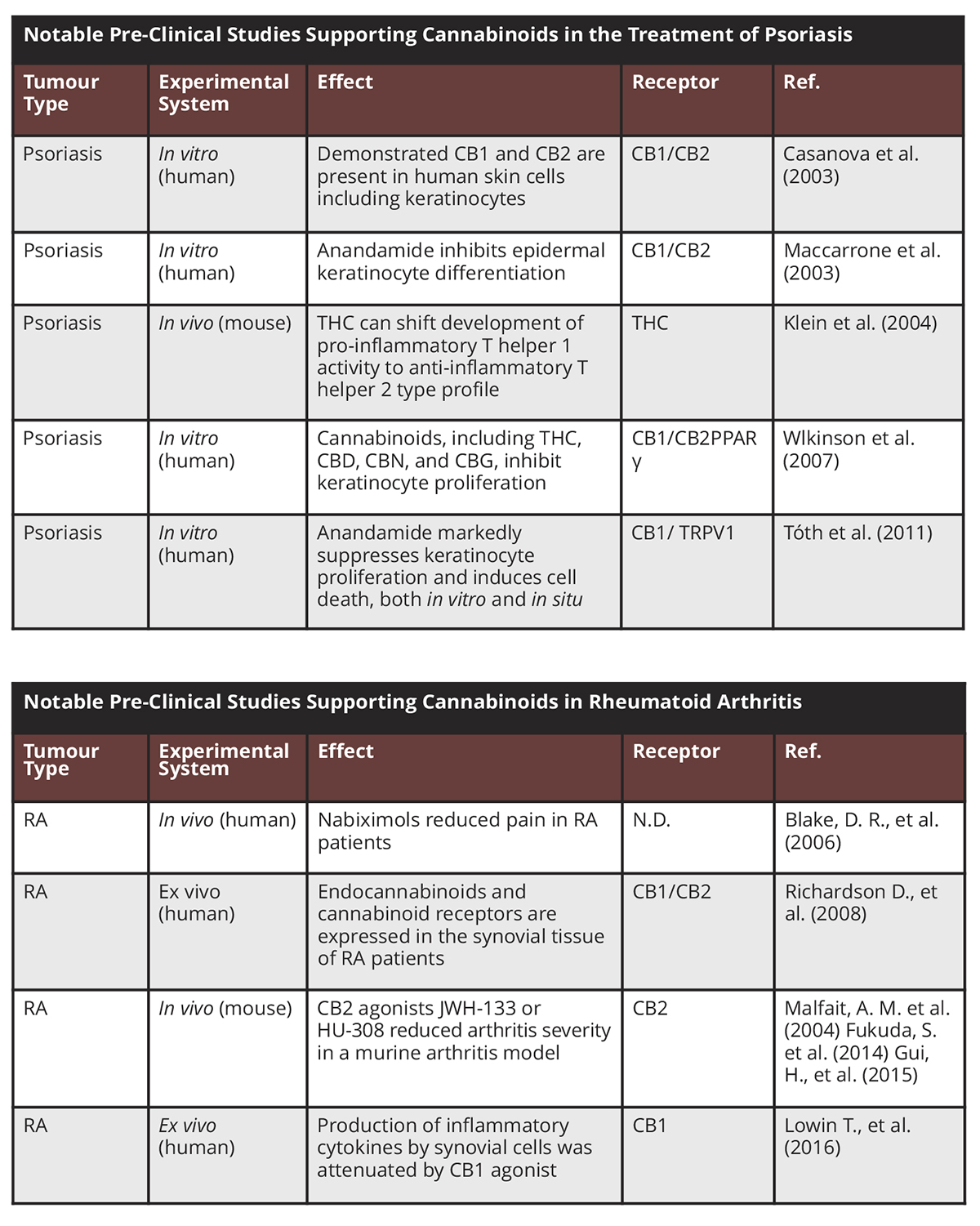
The following pre-clinical studies support the use of cannabinoids in the treatment of psoriasis:
A 2003 study in Journal of Clinical Investigation demonstrated that the cannabinoid receptors CB1 and CB2 are present in human skin cells, including keratinocytes;4
A 2003 study showed that anandamide, an endogenous CB receptor ligand, inhibits epidermal keratinocyte differentiation (abnormal keratinocyte differentiation is a hallmark of psoriasis);5
In 2004, a study in the Journal of Neuroimmunology used an in vivo mouse model to show that THC can shift the development of the predominantly pro-inflammatory T helper 1 (Th1) cell to the more anti-inflammatory (Th2) cell type profile;6
A 2007 study, published in the Journal of Dermatological Science, demonstrated that a range of cannabinoids inhibit keratinocyte proliferation in hyperproliferating human keratinocyte cell lines.7 The cannabinoids inhibited keratinocyte proliferation in a concentration-dependent manner. The activity of CBN (not significantly active at CB1/CB2 receptors) indicates more than one mechanism of action;
In 2011, a study using human cultured keratinocytes and a skin organotypic culture model, provided evidence that anandamide markedly suppresses keratinocyte proliferation and induces cell death, both in vitro and in situ. The cellular actions were mediated by CB1 and transient receptor potential vanilloid-1 (TRPV1). The cellular effects of anandamide are most probably mediated by Ca2+ influx and intracellular accumulation via the non-selective, highly Ca2+-permeable ion channel TRPV1. The study was published in the Journal of Investigative Dermatology;8
A 2016 study, published in the Annals of Dermatology, investigated the effect of CB1 agonists on mast cell activation. The authors found that CB1 agonists inhibited the release of inflammatory mediators and markedly and dose-dependently suppressed cell proliferation.9
Cannabinoids and rheumatoid arthritis
RA is one of the most prevalent autoimmune diseases and one of the main causes of disability globally, causing pain, joint malformation and joint destruction.10 Preliminary evidence suggests that cannabinoids have a role in the future treatment of RA.
In one study,11 protein and mRNA expression of endocannabinoids, AEA and 2-AG, and cannabinoid receptors, CB1 and CB2, were found in synovial tissue obtained from 13 patients diagnosed with RA and undergoing arthroplasty whilst synovial tissue obtained from healthy volunteers was negative for the same endocannabinoids. Another study of synovial tissue from patients with RA12 found that of inflammatory cytokines, IL-6 and IL-8, which are stimulated by synovial cells, were attenuated by low concentrations of the synthetic cannabinoid WIN 55,212-2.
Furthermore, three different research groups achieved improvement in mice with collagen-induced arthritis (“CIA”), following treatment with various cannabinoids;13 The use of cannabinoids for the treatment of pain associated with RA has been assessed in only one 2006 clinical trial, where 58 patients with RA were allocated either nabiximols or a placebo.14 Compared with placebo, patients treated with nabiximols exhibited decreased pain along with improved sleep quality.15
1 Oláh, A., et al. (2017) Targeting Cannabinoid Signalling in the Immune System: ‘High’-ly Exciting Questions, Possibilities, and Challenges. Front Immunol 8:1487.
2 Habif, TP. (2016) Psoriasis and other papulosquamous diseases. Clinical Dermatology. 6th ed. Philadelphia, PA: Elsevier 263-328.
3 van de Kerkhof, PCM and Nestlé, FO (2018) Dermatology. 4th Edition, By Bolognia, JL., et al. 8, Psoriasis 138-160.
4 Casanova, ML., et al. (2003) Inhibition of skin tumour growth and angiogenesis in-vivo by activation of cannabinoid receptors. J Clin Invest 111:43-50.
5 Maccarrone, M., et al. (2003) The endocannabinoid system in human keratinocytes. Evidence that anandamide inhibits epidermal differentiation through CB1 receptor-dependent inhibition of protein kinase C, activation protein-1, and transglutaminase. J Biol Chem 278:33896-33903.
6 Klein, TW., et al. (2004) Cannabinoid receptors and T helper cells. J Neuroimmunol 147:91-94.
7 Wilkinson, JD., et al. (2007) Cannabinoids inhibit human keratinocyte proliferation through a non-CB1/CB2 mechanism and have a potential therapeutic value in the treatment of psoriasis. J Dermatolog Sci 45:87-92.
8 Tóth, BI., et al. (2011) Endocannabinoids modulate human epidermal keratinocyte proliferation and survival via the sequential engagement of cannabinoid receptor-1 and transient receptor potential vanilloid-1. J Invest Dermatol 5:1095-104.
9 Nam, G., et al. (2016) Selective Cannabinoid Receptor-1 Agonists Regulate Mast Cell Activation in an Oxazolone-Induced Atopic Dermatitis Model. Ann Dermatol 28(1):22-9.
10 Shapira, Y., et al. (2010) Geoepidemiology of autoimmune rheumatic diseases. Nat Rev Rheumatol 6:468–476.
11 Richardson, D., et al. (2008) Characterisation of the cannabinoid receptor system in synovial tissue and fluid in patients with osteoarthritis and rheumatoid arthritis. Arthritis Res Ther 10(2):R43.
12 Lowin, T., et al. (2016) The synthetic cannabinoid WIN55,212-2 mesylate decreases the production of inflammatory mediators in rheumatoid arthritis synovial fibroblasts by activating CB2, TRPV1, TRPA1 and yet unidentified receptor targets. J Inflamm 13:15.
13 Malfait, AM., et al. (2000) The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen-induced arthritis. Proc Natl Acad Sci USA 97:9561–9566; Fukuda, S., et al. (2014) Cannabinoid receptor 2 as a potential therapeutic target in rheumatoid arthritis. BMC Musculoskelet Disord 15:275; Gui, H., et al. (2015) Activation of cannabinoid receptor 2 attenuates synovitis and joint destruction in collagen-induced arthritis. Immunobiology 220:817–822.
14 Blake, DR., et al. (2006) Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology 45:50–52.
15 Blake, DR., et al. (2006) Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology 45:50–52.
*Please note: This is a commercial profile








