
Mabel L Rice from the University of Kansas describes how nonverbal cognitive impairments are neither necessary nor sufficient
Children’s language starts out very simply and grows with age. Yet some children do not keep up with their age peers. This is a developmental condition known as “language impairments,” which sometimes but not always exists when children have other developmental disorders, such as hearing loss or cognitive impairments. The cause of children’s language impairments is not known. People often draw upon the observed overlap with other obvious developmental disorders such as hearing loss, intellectual impairments, autism spectrum disorder (ASD), Down syndrome, or Fragile X to conclude that language impairments share the same underlying cause. This assumption, although widespread, is off the mark in important ways and can create misleading impressions of children with language impairments and their families.
Instead, the acquisition of language follows a distinct pathway. This is evident in the documentation of selective sparing of language in children with cognitive impairments and selective impairment of language in children’s development, most notably in children with Specific Language Impairment (SLI). This is the most common, but unrecognized, developmental disorder of childhood, which most likely persists into adulthood for many of the affected children. Best estimates are that 7-10% of children who have no hearing loss or other developmental delays show language impairments at school entry, around 5 years of age (1,2).
The language of children with SLI is not the same as unaffected children, yet also shows many of the same strengths (3). Important features of SLI are that children are not likely to outgrow it, are likely to encounter difficulties in learning to read and likely to struggle in other academic endeavours. People can assume the children may not be very bright or are simply poorly motivated, assumptions that only add to the frustration of children with undiagnosed SLI.
Selective sparing of language acquisition in cases of very limited cognitive abilities
To unpack the relationship between general cognitive ability and language ability, let us begin with cases of selective sparing of language in persons with very limited cognitive abilities. Such children have been documented in the literature for a long time and are of interest to scholars of the origins of human language abilities. For example, one well-documented phenomenon is the “cocktail party syndrome” for some patients (adults or children) with spina bifida and/or hydrocephalus, in which subnormal intelligence co-exists with excessive talking comprised of superficial content but well-formed and sometimes quite complex grammar (4). A detailed case study is reported of an adolescent female referred to as “D.H.” She functioned in everyday life situations at the level of significant cognitive impairments. Yet in her spontaneous conversation, her language appeared to be normal, with appropriate syntax, vocabulary and interactive topic maintenance. The conclusion of the linguists who studied her was that she had skilful use of all aspects of language, in spite of her cognitive impairment, posing a puzzle that persists to the present (4).
Another well-documented case history describes a young man with limited cognitive abilities who had extraordinary linguistic prowess. He was a native speaker of English, with a diagnosis of brain damage of an unknown kind. His performance IQ scores were between 42 and 75 (100 is expected) and his verbal IQ scores were between 89 and 102 (also with 100 as expected). As a young adult, he lived in a sheltered community with assistance with daily living activities. He had a remarkable ability to translate from and communicate in a large number of languages, with some knowledge of Danish, Dutch, Finnish, French, German, Modern Greek, Hindi, Italian, Norwegian, Polish, Portuguese, Russian, Spanish, Swedish, Turkish and Welsh. His linguistic abilities were studied in great detail by linguists hoping to capture the underlying properties of universal grammar that were spared in his condition (5).
Children with ASD are often thought of as having language impairments and limited cognitive abilities. Yet the recent revision of the Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (6) revised the diagnostic criteria for ASD to demote language impairments from a centrally defining characteristic to a “specifier” condition. This means that ASD can be officially diagnosed in children with or without language impairments, and with or without intellectual impairments. Instead, deficits in social communication and social behaviour are crucial to diagnosis, as are restrictive, repetitive patterns of behaviour, interests, or activity. In other words, the DSM-5 criteria recognize that classic language impairments are not intrinsically interconnected with social communication deficits or repetitive behaviours, and are not diagnostic of ASD.
Documentation of independence of language impairments and cognitive impairments in population-based samples of children
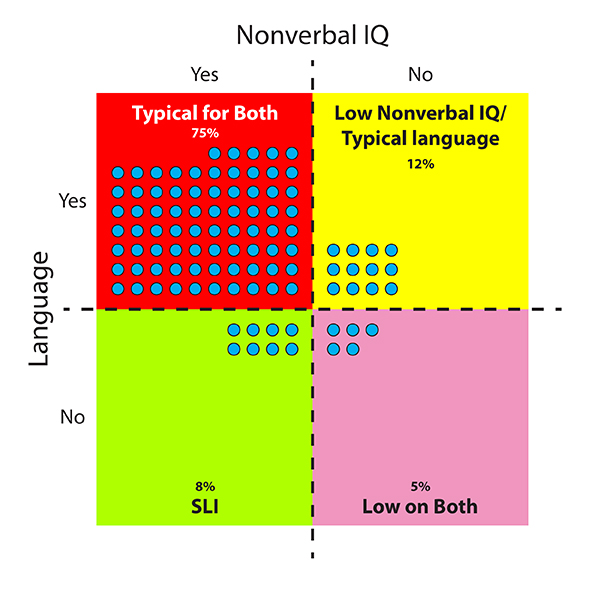
Population-based studies recruit a large sample of children representative of the full range of children in the population. When all children in the sample are measured, it is possible to identify children with SLI and children who have low nonverbal IQ but do not have language impairments. Either of these groups is likely to be unidentified by educators or other special service providers if there is a strong assumption of causal overlap for cognitive impairments and language impairments in children without other obvious developmental disabilities indicative of brain damage or other syndromic conditions. The evidence required to evaluate this possibility is expensive to obtain because assessments should be individually administered to each child for domains of language and nonverbal cognitive abilities. This is time-consuming and requires well-trained data collectors, in addition to experts in experimental design and quantitative analyses. One such study (2,7) is of interest here because measures from the same 5-year-old children are reported for general language assessment, nonverbal IQ, a grammar marker (8), and speech disorders (9). Children were excluded from the sample if they had neurological disorders, clinical syndromes, and/or hearing loss. The outcomes can be presented as percentages of children who fall into four groups based on levels of language ability and nonverbal IQ: 1) Typical or above in both language and nonverbal IQ; 2) Low levels of both language and nonverbal IQ; 3) Typical language and low nonverbal IQ; and 4) Low language and typical or above nonverbal IQ (i.e., a profile consistent with SLI). See another paper (10) for more details about the assessments in the study.
The results are displayed in Figure 1. Two cells, indicated in red and pink, are expected to collect all the children if language and nonverbal IQ are tightly associated with a shared causal pathway. Instead, we see nontrivial exceptions in the off cells: Children with low nonverbal IQ but nevertheless typical or above language scores (~12%) (shown in the yellow cell), and children with SLI (low language with typical or above nonverbal IQ) (~8%) (green cell). The expected red cell of “typical children” captures 75% of the sample; the expected pink cell of low language and nonverbal IQ captures 5% in this sample which excluded children with neurological disorders. So roughly 20% of the children show a profile inconsistent with the assumption that low nonverbal abilities cause SLI. The conclusion is that low nonverbal IQ levels are neither necessary nor sufficient for language impairments in children.
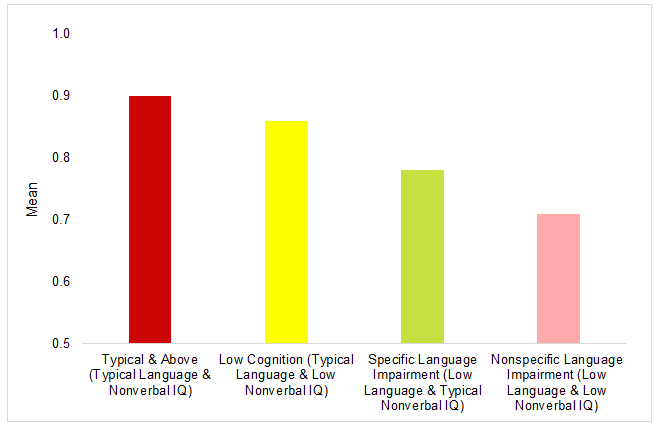
On a more detailed level, there is evidence in support of selective sparing of certain properties of the grammar. English sentences have a requirement for grammatical tense marking (also called “finiteness marking”) for a full clause. This is especially evident in questions with DO, such as “Where does he go?” The form of DO is required to mark tense and agreement with the subject, without any contribution to the meaning of the sentence. Other indicators of grammatical tense marking are copula and auxiliary forms of BE, third person singular -s, regular and irregular forms of past tense (11). Young English-speaking children are likely to use these forms optionally where they are required in sentences for some time before they consistently use them, a period that persists for children with SLI (12,13). Thus, there is a reason to think of this grammatical requirement as “weak” in some children. The results are shown in Figure 2, which reports the mean percentage correct for grammatical tense marking. Five years of age is when typically developing children are reaching full mastery, with a group mean of .90 or 90% use in obligatory contexts as shown in the red bar of the figure. The Low Cognition group is not statistically significantly different, with a mean of .86 (yellow bar). On the other hand, the SLI group scores statistically significantly lower, with a mean of .78 (green bar), and the Low/Low group is lowest, with a mean of .71 (pink bar). The pattern across the groups provides further support to the possibility of selective sparing of grammar in children with low nonverbal IQ even when they do not have classic clinical syndromes associated with a developmental disorder, as documented in the cases above. Thus, the grammar marker of SLI is not diagnostic of low nonverbal IQ.
The assumption that low nonverbal IQ causes SLI could be related to the ways in which children who do not match our expectations can remain undetected. The cases of selective sparing of language can cause people to assume a child has robust nonverbal IQ when this is not true, thereby leading to frustration for the child in a school where a lack of nonverbal ability can be attributed to low motivation or poor study habits. On the other hand, children with SLI often go undetected in part because they develop compensatory ways of avoiding situations that call for more language ability than they have. This can be apparent in their avoidance of advocating for themselves in childhood disputes with peers or avoiding verbal participation in class activities. Another way they remain invisible is that most children with SLI do not have clinically significant speech disorders, even at school entry. In the study reported in Figures 1 and 2, 98.2% of the children had developmentally appropriate speech in a measure adjusted for mild misarticulations, such as a frontal lisp, that may be evident at 5 years but are likely to be outgrown by 7 years of age. The rate of speech impairments in children with SLI was estimated at 0.51%, suggesting that speech disorders and language impairments are likely to appear independently in young children. The rate of speech impairments in the low/low group was 0.77%; in the low nonverbal/typical or above language group the rate was 0.5%. A recent population study also reported high levels of speaking ability in children with language disorders1 although the groupings were not defined out in the same ways as the study reported here, i.e., the prevalence estimates for the low nonverbal IQ group included children who did not have language impairments.
The conclusion is that the common assumption that children with SLI are not very bright is not warranted. Instead, children with SLI can have normal or above nonverbal IQ levels and children with low nonverbal IQ levels can have language abilities as expected for their age. Further, these non-conforming conditions/cells are not rare, comprising about 20% of the population. Language can be selectively impaired or selectively spared. This means scientists need to search for two possible causal pathways that sometimes intersect, instead of one common cause. It also means the common assumption needs to be suspended when encountering children likely to have SLI.
Please note: this is a commercial profile
References
1 Norbury CF, Gooch D, Wray C, et al. The impact of nonverbal ability on prevalence and clinical presentation of language disorder: evidence from a population study. Journal of Child Psychology & Psychiatry. 2016;57(11):1247-1257.
2 Tomblin JB, Records NL, Buckwalter P, Zhang X, Smith E, O’Brien M. The prevalence of specific language impairment in kindergarten children. J Speech Hear Res. 1997;40:1245-1260.
3 Rice ML. Specific language impairment: What do we know? Adjacent Open Access. 2017(August):34-35.
4 Cromer R. A case study of dissociations between language and cognition. In: Tager-Flusberg H, ed. Constraints on language acquisition: Studies of atypical children. New York, NY: Psychology Press; 2014:141-153.
5 Smith N, Tsimpli I-M. The Mind of a Savant: Language Learning and Modularity. Oxford, UK: Blackwell; 1995.
6 Association AP. Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C.: American Psychiatric Association; 2013.
7 Tomblin JB, Smith E, Zhang X. Epidemiology of Specific Language Impairment: Prenatal and perinatal risk factors. J Commun Disord. 1997;30:325-344.
8 Rice ML, Tomblin JB, Hoffman L, Richman WA, Marquis J. Grammatical tense deficits in children with SLI and nonspecific language impairment: Relationships with nonverbal IQ over time. J Speech Lang Hear Res. 2004;47:816-834.
9 Shriberg LD, Tomblin JB, McSweeny JL. Prevalence of speech delay in 6-year-old children and comorbidity with language impairment. J Speech Lang Hear Res. 1999;42:1461-1481.
10 Rice ML. Specific Language Impairment, Nonverbal IQ, ADHD, ASD, Cochlear Implants, Bilingualism and Dialectal Variants: Defining the boundaries, clarifying clinical conditions and sorting out causes. Journal of speech, language, and hearing research: JSLHR. 2016;59:122-132.
11 Quirk R, Greenbaum S, Leech G, Svartvik J. A comprehensive grammar of the English language. New York: Longman, Inc.; 1985.
12 Rice ML, Wexler K. Toward tense as a clinical marker of specific language impairment in English-speaking children. J Speech Hear Res. 1996;39:1239-1257.
13 Rice ML, Wexler K. Rice/Wexler Test of Early Grammatical Impairment. San Antonio, TX: The Psychological Corporation; 2001.
Please note: this is a commercial profile
Mabel L Rice
University of Kansas
Tel: +1 785 864 4570








